PDS Biotech is a clinical-stage immunotherapy company developing a growing pipeline of molecularly targeted cancer and infectious disease immunotherapies based on the Company’s proprietary Versamune® and Infectimune™ T-cell activating technology platforms. Our Versamune®-based products have demonstrated the potential to overcome the limitations of current immunotherapy by inducing in vivo, large quantities of high-quality, highly potent polyfunctional tumor specific CD4+ helper and CD8+ killer T-cells. PDS Biotech has developed multiple therapies, based on combinations of Versamune® and disease-specific antigens, designed to train the immune system to better recognize diseased cells and effectively attack and destroy them. The Company’s pipeline products address various cancers including HPV16-associated cancers (anal, cervical, head and neck, penile, vaginal, vulvar) and breast, colon, lung, prostate and ovarian cancers.
Robert LeBoyer, Vice President, Research Analyst, Life Sciences , Noble Capital Markets, Inc.
Refer to the full report for the price target, fundamental analysis, and rating.
Triple Therapy Advances. PDS Biotech announced that the FDA has agreed to requirements for a registration trial using PDS0101 “Triple Combination” therapy in head and neck cancer. The study will test the combination of PDS0101, PDS0301, and a commercially available checkpoint inhibitor. We believe the changes from the previous trial should make regulatory approval faster, with additional tumor types added after market entry.
New Combination Eliminates An Unapproved Checkpoint Inhibitor. The new Triple Combination uses PDS010 to stimulate an immune response against the HPV antigen, PDS0301 to stimulate a robust immune response, and a checkpoint inhibitor to allow the immune system to recognize the tumor cells. The previous trial included bintrafusp alfa, an experimental checkpoint inhibitor. We believe the change to an approved checkpoint inhibitor simplifies the regulatory path.
Equity Research is available at no cost to Registered users of Channelchek. Not a Member? Click ‘Join’ to join the Channelchek Community. There is no cost to register, and we never collect credit card information.
This Company Sponsored Research is provided by Noble Capital Markets, Inc., a FINRA and S.E.C. registered broker-dealer (B/D).
*Analyst certification and important disclosures included in the full report. NOTE: investment decisions should not be based upon the content of this research summary. Proper due diligence is required before making any investment decision.
MAIA is a targeted therapy, immuno-oncology company focused on the development and commercialization of potential first-in-class drugs with novel mechanisms of action that are intended to meaningfully improve and extend the lives of people with cancer. Our lead program is THIO, a potential first-in-class cancer telomere targeting agent in clinical development for the treatment of NSCLC patients with telomerase-positive cancer cells. For more information, please visit www.maiabiotech.com.
Robert LeBoyer, Vice President, Research Analyst, Life Sciences , Noble Capital Markets, Inc.
Refer to the full report for the price target, fundamental analysis, and rating.
THIO Is A First-In-Class Cancer Therapeutic With A Dual Mechanism Of Action. MAIA Biotechnology is in Phase 2 development with THIO, a drug directed at the telomeres of cancer cell chromosomes. These are structures at the distal tips of the chromosomes that protect the coding DNA regions and have functions needed for DNA replication. THIO is a modified nucleoside analogue that targets the chromosome’s telomeres, leading to cell death, and stimulates the immune system to attack remaining cancer cells.
THIO Is Phase 2 With A Checkpoint Inhibitor. The direct killing and stimulation of an immune response increases the number of immune killing cells in the tumor that can attack remaining cancer cells. Preclinical studies testing THIO in combination with checkpoint inhibitors showed complete killing and long-term durability of its effects. The current Phase 2 clinical trial program is testing THIO in combination with Libtayo, a PD-1 inhibitor from Regeneron, in non-small cell lung cancer (NSCLC).
Equity Research is available at no cost to Registered users of Channelchek. Not a Member? Click ‘Join’ to join the Channelchek Community. There is no cost to register, and we never collect credit card information.
This Company Sponsored Research is provided by Noble Capital Markets, Inc., a FINRA and S.E.C. registered broker-dealer (B/D).
*Analyst certification and important disclosures included in the full report. NOTE: investment decisions should not be based upon the content of this research summary. Proper due diligence is required before making any investment decision.
Microbes in Your Food Can Help or Hinder Your Body’s Defenses Against Cancer – How Diet Influences the Conflict Between Cell ‘Cooperators’ and ‘Cheaters’
The microbes living in your food can affect your risk of cancer. While some help your body fight cancer, others help tumors evolve and grow.
Gut microbes can influence your cancer risk by changing how your cells behave. Many cancer-protective microbes support normal, cooperative behavior of cells. Meanwhile, cancer-inducing microbes undermine cellular cooperation and increase your risk of cancer in the process.
This article was republished with permission from The Conversation, a news site dedicated to sharing ideas from academic experts. It represents the research-based findings and thoughts of Gissel Marquez Alcaraz, Ph.D. Student in Evolutionary Biology, Arizona State University and Athena Aktipis, Associate Professor of Psychology, Center for Evolution and Medicine, Arizona State University.
We are evolutionary biologists who study how cooperation and conflict occur inside the human body, including the ways cancer can evolve to exploit the body. Our systematic review examines how diet and the microbiome affect the ways the cells in your body interact with each other and either increase or decrease your risk of cancer.
Cancer is a Breakdown of Cell Cooperation
Every human body is a symphony of multicellular cooperation. Thirty trillion cells cooperate and coordinate with each other to make us viable multicellular organisms.
For multicellular cooperation to work, cells must engage in behaviors that serve the collective. These include controlled cell division, proper cell death, resource sharing, division of labor and protection of the extracellular environment. Multicellular cooperation is what allows the body to function effectively. If genetic mutations interfere with these proper behaviors, they can lead to the breakdown of cellular cooperation and the emergence of cancer.
Cancer cells can be thought of as cellular cheaters because they do not follow the rules of cooperative behavior. They mutate uncontrollably, evade cell death and take up excessive resources at the expense of the other cells. As these cheater cells replicate, cancer in the body begins to grow.
Cancer is fundamentally a problem of having multiple cells living together in one organism. As such, it has been around since the origins of multicellular life. This means that cancer suppression mechanisms have been evolving for hundreds of millions of years to help keep would-be cancer cells in check. Cells monitor themselves for mutations and induce cell death, also known as apoptosis, when necessary. Cells also monitor their neighbors for evidence of abnormal behavior, sending signals to aberrant cells to induce apoptosis. In addition, the body’s immune system monitors tissues for cancer cells to destroy them.
Cells that are able to evade detection, avoid apoptosis and replicate quickly have an evolutionary advantage within the body over cells that behave normally. This process within the body, called somatic evolution, is what leads cancer cells to grow and make people sick.
Microbes Can Help or Hinder Cell Cooperation
Microbes can affect cancer risk through changing the ways that the cells of the body interact with one another.
Some microbes can protect against cancer by helping maintain a healthy environment in the gut, reducing inflammation and DNA damage, and even by directly limiting tumor growth. Cancer-protective microbes like Lactobacillus pentosus, Lactobacillus gasseri and Bifidobacterium bifidum are found in the environment and different foods, and can live in the gut. These microbes promote cooperation among cells and limit the function of cheating cells by strengthening the body’s cancer defenses. Lactobacillus acidophilus, for example, increases the production of a protein called IL-12 that stimulates immune cells to act against tumors and suppress their growth.
Other microbes can promote cancer by inducing mutations in healthy cells that make it more likely for cellular cheaters to emerge and outcompete cooperative cells. Cancer-inducing microbes such as Enterococcus faecalis, Helicobacter pylori and Papillomavirus are associated with increased tumor burden and cancer progression. They can release toxins that damage DNA, change gene expression and increase the proliferation of tumor cells. Helicobacter pylori, for example, can induce cancer by secreting a protein called Tipα that can penetrate cells, alter their gene expression and drive gastric cancer.
Healthy Diet with Cancer-Protective Microbes
Because what you eat determines the amount of cancer-inducing and cancer-preventing microbes inside your body, we believe that the microbes we consume and cultivate are an important component of a healthy diet.
Beneficial microbes are typically found in fermented and plant-based diets, which include foods like vegetables, fruits, yogurt and whole grains. These foods have high nutritional value and contain microbes that increase the immune system’s ability to fight cancer and lower overall inflammation. High-fiber foods are prebiotic in the sense that they provide resources that help beneficial microbes thrive and subsequently provide benefits for their hosts. Many cancer-fighting microbes are abundantly present in fermented and high-fiber foods.
In contrast, harmful microbes can be found in highly-processed and meat-based diets. The Western diet, for example, contains an abundance of red and processed meats, fried food and high-sugar foods. It has been long known that meat-based diets are linked to higher cancer prevalence, and that red meat is a carcinogen. Studies have shown that meat-based diets are associated with cancer-inducing microbes including Fusobacteria and Peptostreptococcus in both humans and other species.
Microbes can enhance or interfere with how the body’s cells cooperate to prevent cancer. We believe that purposefully cultivating a microbiome that promotes cooperation among our cells can help reduce cancer risk.
Exciting Data from University of Pittsburgh Researchers in Non Human Primates that Underpins Genprex’s Gene Therapy Program in Diabetes to be Showcased
AUSTIN, Texas — (January 4, 2023) — Genprex, Inc. (“Genprex” or the “Company”) (NASDAQ: GNPX), a clinical-stage gene therapy company focused on developing life-changing therapies for patients with cancer and diabetes, today announced that its research collaborators at the University of Pittsburgh will present preclinical data highlighting the therapeutic potential of Genprex’s gene therapy for Type 1 diabetes at the 16th International Conference on Advanced Technologies & Treatments for Diabetes (ATTD 2023) being held February 22-25 in Berlin, Germany and online.
“ATTD 2023 presents an ideal opportunity for the results of this important study to be presented to the diabetes community. The data further support the potential of Genprex’s novel gene therapy being developed for the treatment of Type 1 diabetes to change the trajectory of this devastating disease,” said Mark Berger, MD, Genprex’s Chief Medical Officer. “Using the expression of Pdx1 and MafA transcription factors, this approach has been shown first in mice and then in non human primate studies to lead to the creation of new beta-like cells that produce insulin and may provide long-term replacement of beta-cells.”
The diabetes gene therapy approach is comprised of a novel infusion process that uses endoscopic delivery of an adeno-associated virus (AAV) vector to bring therapeutic genes directly to the pancreas. In models of Type 1 diabetes, these genes express proteins that transform alpha cells in the pancreas into functional beta-like cells, which can produce insulin but are distinct enough from beta cells to evade the body’s immune system. In Type 2 diabetes, where autoimmunity is not at play, it is believed that using a similar approach the exhausted beta cells will be rejuvenated and replenished.
Presentation Details:
Abstract Number: 203
Abstract Title: Pancreatic Intraductal Infusion of Adeno-Associated Virus To Treat Non-Human Primates in a Toxin-Induced Diabetes Model
Format: Oral Presentation
Presenter: Ranjeet Kalsi, DO, representing the laboratory of George Gittes, MD, Professor of Surgery and Pediatrics and Chief of the Division of Pediatric Surgery, University of Pittsburgh School of Medicine
Time/Date: 1:45 pm Central European Standard Time on Saturday, February 25, 2023
The abstract will be made available on the ATTD conference website at https://attd.kenes.com.
About Genprex, Inc.
Genprex, Inc. is a clinical-stage gene therapy company focused on developing life-changing therapies for patients with cancer and diabetes. Genprex’s technologies are designed to administer disease-fighting genes to provide new therapies for large patient populations with cancer and diabetes who currently have limited treatment options. Genprex works with world-class institutions and collaborators to develop drug candidates to further its pipeline of gene therapies in order to provide novel treatment approaches. Genprex’s oncology program utilizes its proprietary, non-viral ONCOPREX® Nanoparticle Delivery System, which the Company believes is the first systemic gene therapy delivery platform used for cancer in humans. ONCOPREX encapsulates the gene-expressing plasmids using lipid nanoparticles. The resultant product is administered intravenously, where it is then taken up by tumor cells that express tumor suppressor proteins that are deficient in the body. The Company’s lead product candidate, REQORSA® (quaratusugene ozeplasmid), is being evaluated as a treatment for non-small cell lung cancer (NSCLC) (with each of these clinical programs receiving a Fast Track Designation from the Food and Drug Administration) and for small cell lung cancer. Genprex’s diabetes gene therapy approach is comprised of a novel infusion process that uses an endoscope and an adeno-associated virus (AAV) vector to deliver Pdx1 and MafA genes to the pancreas. In models of Type 1 diabetes, the genes express proteins that transform alpha cells in the pancreas into functional beta-like cells, which can produce insulin but are distinct enough from beta cells to evade the body’s immune system. In a similar approach used in Type 2 diabetes, where autoimmunity is not at play, it is believed that exhausted beta cells are rejuvenated and replenished.
Cautionary Language Concerning Forward-Looking Statements
Statements contained in this press release regarding matters that are not historical facts are “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995. These forward-looking statements are made on the basis of the current beliefs, expectations and assumptions of management, are not guarantees of performance and are subject to significant risks and uncertainty. These forward-looking statements should, therefore, be considered in light of various important factors, including those set forth in Genprex’s reports that it files from time to time with the Securities and Exchange Commission and which you should review, including those statements under “Item 1A – Risk Factors” in Genprex’s Annual Report on Form 10-K for the year ended December 31, 2021.
Because forward-looking statements are subject to risks and uncertainties, actual results may differ materially from those expressed or implied by such forward-looking statements. Such statements include, but are not limited to, statements regarding: the timing and success of Genprex’s clinical trials and regulatory approvals, including the extent and impact of the COVID-19 pandemic; the effect of Genprex’s product candidates, alone and in combination with other therapies, on cancer and diabetes; Genprex’s future growth and financial status; Genprex’s commercial and strategic partnerships, including those with its third party manufacturers and their ability to successfully perform and scale up the manufacture of its product candidates; and Genprex’s intellectual property and licenses.
These forward-looking statements should not be relied upon as predictions of future events and Genprex cannot assure you that the events or circumstances discussed or reflected in these statements will be achieved or will occur. If such forward-looking statements prove to be inaccurate, the inaccuracy may be material. You should not regard these statements as a representation or warranty by Genprex or any other person that Genprex will achieve its objectives and plans in any specified timeframe, or at all. You are cautioned not to place undue reliance on these forward-looking statements, which speak only as of the date of this press release. Genprex disclaims any obligation to publicly update or release any revisions to these forward-looking statements, whether as a result of new information, future events or otherwise, after the date of this press release or to reflect the occurrence of unanticipated events, except as required by law.
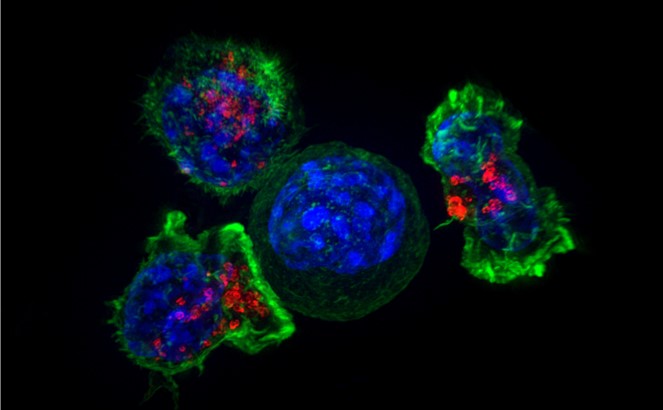
Image: Killer T Cells Surround Cancer Cell – NICHD (Flickr)
Anti-Cancer CAR-T Therapy Reengineers T-cells to Kill Tumors – and Researchers are Expanding the Limited Types of Cancer it Can Target
Teaching the body’s immune cells to recognize and fight cancer is one of the holy grails in medicine. Over the past two decades, researchers have developed new immunotherapy drugs that stimulate a patient’s immune cells to significantly shrink or even eliminate tumors. These treatments often focus on increasing the cancer-killing ability of cytotoxic T cells. However, these treatments appear to only work for the small group of patients who already have T cells within their tumors. One 2019 study estimated that under 13% of cancer patients responded to immunotherapy.
To bring the benefits of immunotherapy to more patients, scientists have turned to synthetic biology, a new field of study that seeks to redesign nature with new and more useful functions. Researchers have been developing a novel type of therapy that directly gives patients a new set of T cells engineered to attack tumors: chimeric antigen receptor T cells, or CAR-T cells for short.
This article was republished with permission from The Conversation, a news site dedicated to sharing ideas from academic experts. It represents the research-based findings and thoughts of, Gregory Allen, Assistant Professor of Medicine, the University of California, San Francisco.
As an oncology physician and researcher, I believe that CAR-T cell therapy has the potential to transform cancer treatment. It’s already being used to treat lymphoma and multiple myeloma, and has shown remarkable response rates where other treatments have failed.
However, similar success against certain types of tumors such as lung or pancreatic cancer has been slower to develop because of the unique obstacles they put up against T cells. In our newly published research, my colleagues and I have found that adding a synthetic circuit to CAR-T cells could potentially help them bypass the barriers that tumors put up and enhance their ability to eliminate more types of cancer.
How Does CAR-T Cell Therapy Work?
CAR-T cell therapy starts with doctors isolating a patient’s T cells from a sample of their blood. These T cells are then taken back to the lab, where they are genetically engineered to produce a chimeric antigen receptor, or CAR.
CARs are synthetic receptors specifically designed to redirect T cells from their usual targets have them recognize and hone in on tumor cells. On the outside of a CAR is a binder that allows the T cell to stick to tumor cells. Binding to a tumor cell activates the engineered T cell to kill and produce inflammatory cytokines proteins that support T cell growth and function and boost their cancer-killing
CAR-T therapy involves engineering a patient’s own T cells to attack their cancer. National Cancer Institute (NCI)
These CAR-T cells are then stimulated to divide into large numbers over seven to 10 days, then given back to the patient via infusion. The infusion process usually takes place at a hospital where clinicians can monitor for signs of an overactive immune response against tumors, which can be deadly for the patient.
Driving T Cells Into Solid Tumors
While CAR-T cell therapy has seen success in blood cancers, it has faced hurdles when fighting what are called solid tumor cancers like pancreatic cancer and melanoma. Unlike cancers that begin in the blood, these types of cancers grow into a solid mass that produces a microenvironment of molecules, cells and structures that prevent T cells from entering into the tumor and triggering an immune response. Here, even CAR-T cells engineered to specifically target a patient’s unique tumor are unable to access it, suppressing their ability to kill tumor cells.
For the synthetic biology community, the failures of the first generation of CAR-T cell therapy was a call to action to develop a new family of synthetic receptors to tackle the unique challenges solid tumors posed. In 2016, my colleagues in the Lim Lab at the University of California, San Francisco developed a new synthetic receptor that could complement the first CAR design. This receptor, called synthetic Notch receptor, or synNotch, is based on the natural form of Notch in the body, which plays an important role in organ development across many species.
Similar to CARs, the outside of synNotch has a binder that allows T cells to stick to tumor cells. Unlike CARs, the inside of synNotch has a protein that is released when a T cell binds to the tumor. This protein, or transcription factor, allows researchers to better control the T cell by inducing it to produce a specific protein.
For example, one of the most useful applications of synNotch thus far has been to use it to ensure that engineered T cells are only activated when bound to a tumor cell and not healthy cells. Because a CAR may bind to both tumor and healthy cells and induce T cells to kill both, my colleagues engineered T cells that are only activated when both synNotch and CAR are bound to the tumor cell. Because T cells now require both CAR and synNotch receptors to recognize tumors, this increases the precision of T cell killing.
We wondered if we could use synNotch to improve CAR-T cell activity against solid tumors by inducing them to produce more of the inflammatory cytokines, such as IL-2, that enable them to kill tumor cells. Researchers have made many attempts to provide extra IL-2 to help CAR-T cells clear tumors. But because these cytokines are highly toxic, there is a limit to how much IL-2 a patient can safely tolerate, limiting their use as a drug.
So we designed CAR-T cells to produce IL-2 using synNotch. Now, when a CAR-T cell encounters a tumor, it produces IL-2 within the tumor instead of outside it, avoiding causing harm to surrounding healthy cells. Because synNotch is able to bypass the barriers tumors put up, it is able to help T cells amp up and maintain the amount of IL-2 they can make, allowing the T cells to keep functioning even in a hostile microenvironment.
We tested our CAR-T cells modified with synNotch on mice with pancreatic cancer and melanoma. We found that CAR-T cells with synNotch-induced IL-2 were able to produce enough extra IL-2 to overcome the tumors’ defensive barriers and fully activate, completely eliminating the tumors. While all of the mice receiving synNotch modified CAR-T cells survived, none of the CAR-T-only mice did.
Furthermore, our synNotch modified CAR-T cells were able to trigger IL-2 production without causing toxicity to healthy cells in the rest of the body. This suggests that our method of engineering T cells to produce this toxic cytokine only where it is needed can help improve the effectiveness of CAR-T cells against cancer while reducing side effects.
Next Steps
Fundamental questions remain on how this work in mice will translate to people. Our group is currently conducting more studies on using CAR-T cells with synNotch to produce IL-2, with the goal of entering early stage clinical trials to examine its safety and efficacy in patients with pancreatic cancer.
Our findings are one example of how advances in synthetic biology make it possible to engineer solutions to the most fundamental challenges in medicine.
Corporate Presentation to Highlight Company’s Gene Therapies for Cancer and Diabetes
AUSTIN, Texas — (December 2, 2022) — Genprex, Inc. (“Genprex” or the “Company”) (NASDAQ: GNPX), a clinical-stage gene therapy company focused on developing life-changing therapies for patients with cancer and diabetes, today announced that its Executive Vice President, General Counsel and Chief Strategy Officer, Catherine Vaczy, will be providing an overview of the Company’s gene therapies for cancer and diabetes at the following investor conference in December 2022.
Ms. Vaczy will be available for Q&A following the presentation and for in-person one-on-one meetings with investors at the RHK Disruptive Growth Conference.
About Genprex, Inc.
Genprex, Inc. is a clinical-stage gene therapy company focused on developing life-changing therapies for patients with cancer and diabetes. Genprex’s technologies are designed to administer disease-fighting genes to provide new therapies for large patient populations with cancer and diabetes who currently have limited treatment options. Genprex works with world-class institutions and collaborators to develop drug candidates to further its pipeline of gene therapies in order to provide novel treatment approaches. Genprex’s oncology program utilizes its proprietary, non-viral ONCOPREX® Nanoparticle Delivery System, which the Company believes is the first systemic gene therapy delivery platform used for cancer in humans. ONCOPREX encapsulates the gene-expressing plasmids using lipid nanoparticles. The resultant product is administered intravenously, where it is then taken up by tumor cells that express tumor suppressor proteins that are deficient in the body. The Company’s lead product candidate, REQORSA™ (quaratusugene ozeplasmid), is being evaluated as a treatment for non-small cell lung cancer (NSCLC) (with each of these clinical programs receiving a Fast Track Designation from the Food and Drug Administration) and for small cell lung cancer. Genprex’s diabetes gene therapy approach is comprised of a novel infusion process that uses an endoscope and an adeno-associated virus (AAV) vector to deliver Pdx1 and MafA genes to the pancreas. In models of Type 1 diabetes, the genes express proteins that transform alpha cells in the pancreas into functional beta-like cells, which can produce insulin but are distinct enough from beta cells to evade the body’s immune system. In Type 2 diabetes, where autoimmunity is not at play, it is believed that exhausted beta cells are also rejuvenated and replenished.
Cautionary Language Concerning Forward-Looking Statements
Statements contained in this press release regarding matters that are not historical facts are “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995. These forward-looking statements are made on the basis of the current beliefs, expectations and assumptions of management, are not guarantees of performance and are subject to significant risks and uncertainty. These forward-looking statements should, therefore, be considered in light of various important factors, including those set forth in Genprex’s reports that it files from time to time with the Securities and Exchange Commission and which you should review, including those statements under “Item 1A – Risk Factors” in Genprex’s Annual Report on Form 10-K for the year ended December 31, 2021.
Because forward-looking statements are subject to risks and uncertainties, actual results may differ materially from those expressed or implied by such forward-looking statements. Such statements include, but are not limited to, statements regarding: the timing and success of Genprex’s clinical trials and regulatory approvals, including the extent and impact of the COVID-19 pandemic; the effect of Genprex’s product candidates, alone and in combination with other therapies, on cancer and diabetes; Genprex’s future growth and financial status; Genprex’s commercial and strategic partnerships, including those with its third party manufacturers and their ability to successfully perform and scale up the manufacture of its product candidates; and Genprex’s intellectual property and licenses.
These forward-looking statements should not be relied upon as predictions of future events and Genprex cannot assure you that the events or circumstances discussed or reflected in these statements will be achieved or will occur. If such forward-looking statements prove to be inaccurate, the inaccuracy may be material. You should not regard these statements as a representation or warranty by Genprex or any other person that Genprex will achieve its objectives and plans in any specified timeframe, or at all. You are cautioned not to place undue reliance on these forward-looking statements, which speak only as of the date of this press release. Genprex disclaims any obligation to publicly update or release any revisions to these forward-looking statements, whether as a result of new information, future events or otherwise, after the date of this press release or to reflect the occurrence of unanticipated events, except as required by law.
PDS Biotech is a clinical-stage immunotherapy company developing a growing pipeline of molecularly targeted cancer and infectious disease immunotherapies based on the Company’s proprietary Versamune® and Infectimune™ T-cell activating technology platforms. Our Versamune®-based products have demonstrated the potential to overcome the limitations of current immunotherapy by inducing in vivo, large quantities of high-quality, highly potent polyfunctional tumor specific CD4+ helper and CD8+ killer T-cells. PDS Biotech has developed multiple therapies, based on combinations of Versamune® and disease-specific antigens, designed to train the immune system to better recognize diseased cells and effectively attack and destroy them. The Company’s pipeline products address various cancers including HPV16-associated cancers (anal, cervical, head and neck, penile, vaginal, vulvar) and breast, colon, lung, prostate and ovarian cancers.
Robert LeBoyer, Vice President, Research Analyst, Life Sciences , Noble Capital Markets, Inc.
Refer to the full report for the price target, fundamental analysis, and rating.
Raising Our Price Target to $19 Per Share. Data presentations from clinical trials for PDS0101 have driven PDSB within 10% of our previous price target. We continue to see PDS0101 as a highly promising treatment for HPV-positive cancers and see several important milestones to drive the stock higher in the coming year.
Price Target Is Based On PDS010 Sales Potential. Our new price target is based on discounted sales estimates for PDS010 sales in HPV-positive cancer. Following an End-of-Phase 2 meeting with the FDA following the June 2022 VERSATILE-002 data presentation, the company announced that it was accelerating its timetable for the pivotal trial for PDS0101. We expect this trial to begin in 2023 and project product launch in 2026.
Equity Research is available at no cost to Registered users of Channelchek. Not a Member? Click ‘Join’ to join the Channelchek Community. There is no cost to register, and we never collect credit card information.
This Company Sponsored Research is provided by Noble Capital Markets, Inc., a FINRA and S.E.C. registered broker-dealer (B/D).
*Analyst certification and important disclosures included in the full report. NOTE: investment decisions should not be based upon the content of this research summary. Proper due diligence is required before making any investment decision.
PDS Biotech is a clinical-stage immunotherapy company developing a growing pipeline of molecularly targeted cancer and infectious disease immunotherapies based on the Company’s proprietary Versamune® and Infectimune™ T-cell activating technology platforms. Our Versamune®-based products have demonstrated the potential to overcome the limitations of current immunotherapy by inducing in vivo, large quantities of high-quality, highly potent polyfunctional tumor specific CD4+ helper and CD8+ killer T-cells. PDS Biotech has developed multiple therapies, based on combinations of Versamune® and disease-specific antigens, designed to train the immune system to better recognize diseased cells and effectively attack and destroy them. The Company’s pipeline products address various cancers including HPV16-associated cancers (anal, cervical, head and neck, penile, vaginal, vulvar) and breast, colon, lung, prostate and ovarian cancers.
Robert LeBoyer, Vice President, Research Analyst, Life Sciences , Noble Capital Markets, Inc.
Refer to the full report for the price target, fundamental analysis, and rating.
Financial Results Reported With Full Data. PDS Biotech reported a 3Q22 loss of $7.4 million or $(0.26) per share, with cash on September 30 of $71.6 million. PDS Management reviewed two presentations at last week’s Society for Immunotherapy of Cancer (SITC) meeting, providing additional information to the data published in the abstracts. These data continue to show improved efficacy for PDS0101 over current treatments.
Data From Two Studies Was Presented At SITC. As discussed in our Research Note on November 8, the response rate and patient survival for the Phase 2 IMMUNOCERV trial in cervical cancer exceeded the standard of care. Data presented from the Phase 2 Triple Therapy trial showed anti-tumor action by PDS0101, with increases in immune response markers against the tumors and decreases in markers of immune suppression.
This Company Sponsored Research is provided by Noble Capital Markets, Inc., a FINRA and S.E.C. registered broker-dealer (B/D).
*Analyst certification and important disclosures included in the full report. NOTE: investment decisions should not be based upon the content of this research summary. Proper due diligence is required before making any investment decision.
Onconova Therapeutics is a clinical-stage biopharmaceutical company focused on discovering and developing novel products for patients with cancer. The Company has proprietary targeted anti-cancer agents designed to disrupt specific cellular pathways that are important for cancer cell proliferation. Onconova’s novel, proprietary multi-kinase inhibitor narazaciclib (formerly ON 123300) is being evaluated in two Phase 1 dose-escalation and expansion studies. These trials are currently underway in the United States and China. Onconova’s product candidate rigosertib is being studied in an investigator-sponsored study program, including in a dose-escalation and expansion Phase 1/2a investigator-sponsored study with oral rigosertib in combination with nivolumab for patients with KRAS+ non-small cell lung cancer.
Robert LeBoyer, Vice President, Research Analyst, Life Sciences , Noble Capital Markets, Inc.
Refer to the full report for the price target, fundamental analysis, and rating.
3Q22 Showed Continued Progress In Ongoing Trials. Onconova announced a loss of $5.4 million or $(0.26) per quarter for 3Q22, ending the quarter with $42.6 million in cash. In addition to updates on its current clinical trials, the company announced its intentions to start a new Phase 1/2a trial testing narazaciclib in low-grade endometrioid endometrial cancer (LGEEC). This new trial is expected to begin in 1Q23 with first data announced in 4Q23.
New Trial Planned In Endometrial Cancer. The Phase 1/2a trial will test the combination of narazaciclib with letrozole (Femara, an aromatase inhibitor from Novartis) in recurrent low-grade endometrioid endometrial cancer (LGEEC). The trial will start with safety cohorts testing the combination, with a 200 mg dose of narazaciclib with the standard 2.5 mg dose of letrozole. This is the narazaciclib dose that is in its fifth cohort in the Phase 1 trial for solid tumors.
This Company Sponsored Research is provided by Noble Capital Markets, Inc., a FINRA and S.E.C. registered broker-dealer (B/D).
*Analyst certification and important disclosures included in the full report. NOTE: investment decisions should not be based upon the content of this research summary. Proper due diligence is required before making any investment decision.
How Cancer Cells can Become Immortal – New Research Finds a Mutated Gene that Helps Melanoma Defeat the Normal Limits on Repeated Replication
A defining characteristic of cancer cells is their immortality. Usually, normal cells are limited in the number of times they can divide before they stop growing. Cancer cells, however, can overcome this limitation to form tumors and bypass “mortality” by continuing to replicate.
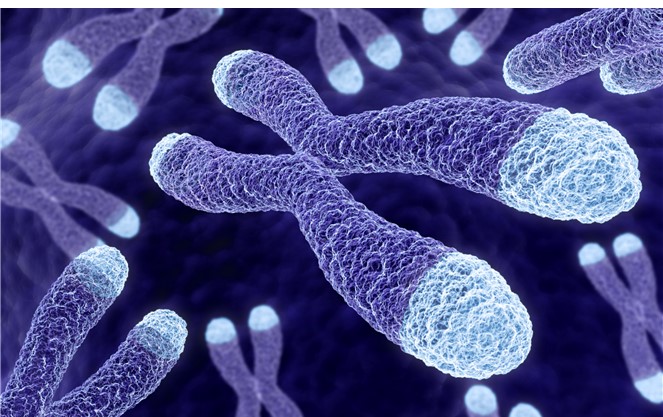
Telomeres play an essential role in determining how many times a cell can divide. These repetitive sequences of DNA are located at the ends of chromosomes, structures that contain genetic information. In normal cells, continued rounds of replication shorten telomeres until they become so short that they eventually trigger the cell to stop replicating. In contrast, tumor cells can maintain the lengths of their telomeres by activating an enzyme called telomerase that rebuilds telomeres during each replication.
Telomeres are protective caps at the ends of chromosomes
Telomerase is encoded by a gene called TERT, one of the most frequently mutated genes in cancer. TERT mutations cause cells to make a little too much telomerase and are thought to help cancer cells keep their telomeres long even though they replicate at high rates. Melanoma, an aggressive form of skin cancer, is highly dependent on telomerase to grow, and three-quarters of all melanomas acquire mutations in telomerase. These same TERT mutations also occur across other cancer types.
Unexpectedly, researchers found that TERT mutations could only partially explain the longevity of telomeres in melanoma. While TERT mutations did indeed extend the life span of cells, they did not make them immortal. That meant there must be something else that helps telomerase allow cells to grow uncontrollably. But what that “second hit” might be has been unclear.
This article was republished with permission from The Conversation, a news site dedicated to sharing ideas from academic experts. It represents the research-based findings and thoughts of Pattra Chun-OnPh.D. Candidate in Environmental and Occupational Health, University of Pittsburgh Health Sciences and Jonathan AlderAssistant Professor of Medicine, University of Pittsburgh Health Sciences.
We are researchers who study the role telomeres play in human health and diseases like cancer in the Alder Lab at the University of Pittsburgh. While investigating the ways that tumors maintain their telomeres, we and our colleagues found another piece to the puzzle: another telomere-associated gene in melanoma.
Cell Immortality Gets a Boost
Our team focused on melanoma because this type of cancer is linked to people with long telomeres. We examined DNA sequencing data from hundreds of melanomas, looking for mutations in genes related to telomere length.
We identified a cluster of mutations in a gene called TPP1. This gene codes for one of the six proteins that form a molecular complex called shelterin that coats and protects telomeres. Even more interesting is the fact that TPP1 is known to activate telomerase. Identifying the TPP1 gene’s connection to cancer telomeres was, in a way, obvious. After all, it was more than a decade ago that researchers showed that TPP1 would increase telomerase activity.
We tested whether having an excess of TPP1 could make cells immortal. When we introduced just TPP1 proteins into cells, there was no change in cell mortality or telomere length. But when we introduced TERT and TPP1 proteins at the same time, we found that they worked synergistically to cause significant telomere lengthening.
To confirm our hypothesis, we then inserted TPP1 mutations into melanoma cells using CRISPR-Cas9 genome editing. We saw an increase in the amount of TPP1 protein the cells made, and a subsequent increase in telomerase activity. Finally, we returned to the DNA sequencing data and found that 5% of all melanomas have a mutation in both TERT and TPP1. While this is still a significant proportion of melanomas, there are likely other factors that contribute to telomere maintenance in this cancer.
Our findings imply that TPP1 is likely one of the missing puzzle pieces that boost telomerase’s capacity to maintain telomeres and support tumor growth and immortality.
Making Cancer Mortal
Knowing that cancer use these genes in their replication and growth means that researchers could also block them and potentially stop telomeres from lengthening and make cancer cells mortal. This discovery not only gives scientists another potential avenue for cancer treatment but also draws attention to an underappreciated class of mutations outside the traditional boundaries of genes that can play a role in cancer diagnostics.
A Blood Test that Screens for Multiple Cancers at Once Promises to Boost Early Detection
Detecting cancer early before it spreads throughout the body can be lifesaving. This is why doctors recommend regular screening for several common cancer types, using a variety of methods. Colonoscopies, for example, screen for colon cancer, while mammograms screen for breast cancer.
While important, getting all these tests done can be logistically challenging, expensive and sometimes uncomfortable for patients. But what if a single blood test could screen for most common cancer types all at once?
This is the promise of multicancer early detection tests, or MCEDs. This year, President Joe Biden identified developing MCED tests as a priority for the Cancer Moonshot, a US$1.8 billion federal effort to reduce the cancer death rate and improve the quality of life of cancer survivors and those living with cancer.
This article was republished with permission from The Conversation, a news site dedicated to sharing ideas from academic experts. It represents the research-based findings and thoughts of Colin Pritchard, Professor of Laboratory Medicine and Pathology, University of Washington.
As a laboratory medicine physician and researcher who develops molecular tests for cancer, I believe MCED tests are likely to transform cancer screening in the near future, particularly if they receive strong federal support to enable rapid innovation.
How MCED Tests Work
All cells in the body, including tumor cells, shed DNA into the bloodstream when they die. MCED tests look for the trace amounts of tumor DNA in the bloodstream. This circulating “cell-free” DNA contains information about what type of tissue it came from and whether it is normal or cancerous.
Testing to look for circulating tumor DNA in the blood is not new. These liquid biopsies – a fancy way of saying blood tests – are already widely used for patients with advanced-stage cancer. Doctors use these blood tests to look for mutations in the tumor DNA that help guide treatment. Because patients with late-stage cancer tend to have a large amount of tumor DNA circulating in the blood, it’s relatively easy to detect the presence of these genetic changes.
MCED tests are different from existing liquid biopsies because they are trying to detect early-stage cancer, when there aren’t that many tumor cells yet. Detecting these cancer cells can be challenging early on because noncancer cells also shed DNA into the bloodstream. Since most of the circulating DNA in the bloodstream comes from noncancer cells, detecting the presence of a few molecules of cancer DNA is like finding a needle in a haystack.
Making things even more difficult, blood cells shed abnormal DNA naturally with aging, and these strands can be confused for circulating cancer DNA. This phenomenon, known as clonal hematopoiesis, confounded early attempts at developing MCED tests, with too many false positive results.
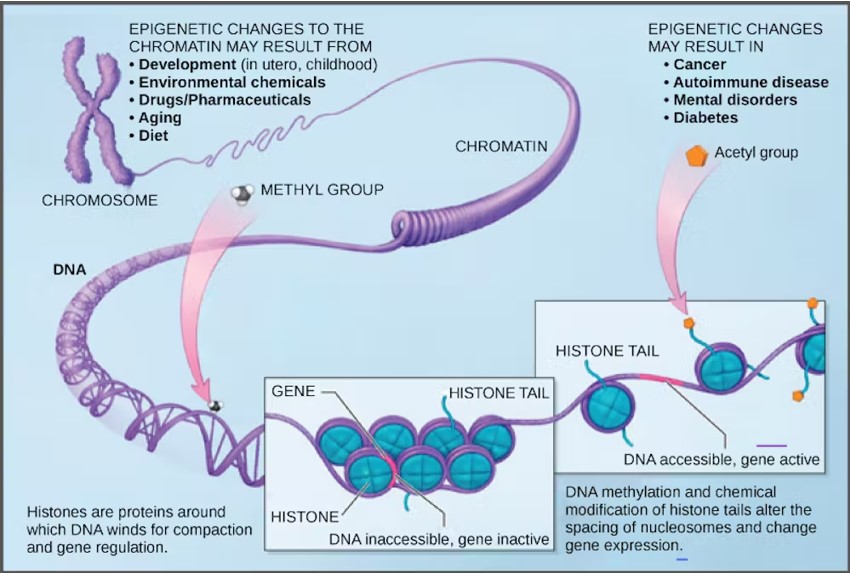
Fortunately, newer tests are able to avoid blood cell interference by focusing on a type of “molecular barcode” embedded in the cancer DNA that identifies the tissue it came from. These barcodes are a result of DNA methylation, naturally existing modifications to the surface of DNA that vary for each type of tissue in the body. For example, lung tissue has a different DNA methylation pattern than breast tissue. Furthermore, cancer cells have abnormal DNA methylation patterns that correlate with cancer type. By cataloging different DNA methylation patterns, MCED tests can focus on the sections of DNA that distinguish between cancerous and normal tissue and pinpoint the cancer’s origin site.
DNA contains molecular patterns that indicate where in the body it came from. (CNX OpenStax/Wikimedia Commons)
Testing Options
There are currently several MCED tests in development and in clinical trials. No MCED test is currently FDA-approved or recommended by medical societies.
In 2021, the biotech company GRAIL, LLC launched the first commercially available MCED test in the U.S. Its Galleri test claims to detect over 50 different types of cancers. At least two other U.S.-based companies, Exact Sciences and Freenome, and one Chinese company, Singlera Genomics, have tests in development. Some of these tests use different cancer detection methods in addition to circulating tumor DNA, such as looking for cancer-associated proteins in blood.
MCED tests are not yet typically covered by insurance. GRAIL’s Galleri test is currently priced at $949, and the company offers a payment plan for people who have to pay out of pocket. Legislators have introduced a bill in Congress to provide Medicare coverage for MCED tests that obtain FDA approval. It is unusual for Congress to consider legislation devoted to a single lab test, and this highlights both the scale of the medical market for MCED and concerns about disparities in access without coverage for these expensive tests.
How Should MCED Tests be Used?
Figuring out how MCED tests should be implemented in the clinic will take many years. Researchers and clinicians are just beginning to address questions on who should be tested, at what age, and how past medical and family history should be taken into account. Setting guidelines for how doctors will further evaluate positive MCED results is just as important.
There is also concern that MCED tests may result in overdiagnoses of low-risk, asymptomatic cancers better left undetected. This happened with prostate cancer screening. Previously, guidelines recommended that all men ages 55 to 69 regularly get blood tests to determine their levels of PSA, a protein produced by cancerous and noncancerous prostate tissue. But now the recommendation is more nuanced, with screening suggested on an individual basis that takes into account personal preferences.
Another concern is that further testing to confirm positive MCED results will be costly and a burden to the medical system, particularly if a full-body scan is required. The out-of-pocket cost for an MRI, for example, can run up to thousands of dollars. And patients who get a positive MCED result but are unable to confirm the presence of cancer after extensive imaging and other follow-up tests may develop lifelong anxiety about a potentially missed diagnosis and continue to take expensive tests in fruitless search for a tumor.
Despite these concerns, early clinical studies show promise. A 2020 study of over 10,000 previously undiagnosed women found 26 of 134 women with a positive MCED test were confirmed to have cancer. A 2021 study sponsored by GRAIL found that half of the over 2,800 patients with a known cancer diagnosis had a positive MCED test and only 0.5% of people confirmed to not have cancer had a false positive test. The test performed best for patients with more advanced cancers but did detect about 17% of the patients who had very-early-stage disease.
MCED tests may soon revolutionize the way clinicians approach cancer screening. The question is whether the healthcare system is ready for them.
PDS Biotech is a clinical-stage immunotherapy company developing a growing pipeline of molecularly targeted cancer and infectious disease immunotherapies based on the Company’s proprietary Versamune® and Infectimune™ T-cell activating technology platforms. Our Versamune®-based products have demonstrated the potential to overcome the limitations of current immunotherapy by inducing in vivo, large quantities of high-quality, highly potent polyfunctional tumor specific CD4+ helper and CD8+ killer T-cells. PDS Biotech has developed multiple therapies, based on combinations of Versamune® and disease-specific antigens, designed to train the immune system to better recognize diseased cells and effectively attack and destroy them. The Company’s pipeline products address various cancers including HPV16-associated cancers (anal, cervical, head and neck, penile, vaginal, vulvar) and breast, colon, lung, prostate and ovarian cancers.
Robert LeBoyer, Vice President, Research Analyst, Life Sciences , Noble Capital Markets, Inc.
Refer to the full report for the price target, fundamental analysis, and rating.
Roundtable Discussion of Head and Neck Cancer. PDS Biotech held a Head and Neck Cancer Roundtable with KOLs to discuss treatments and PDS0101. Although no new data was released, there was a discussion of the cancer, its prognosis, the drugs, and adverse events that showed the need for a new treatment like PDS0101.
Head and Neck Cancer Discussion Included Incidence and Market Size. The presentations discussed the patient population, current drugs, survival and recurrence rates. Newly diagnosed cases of head and neck cancer are often associated with HPV, in contrast to previous generations when it was associated with tobacco and alcohol. Although vaccinations against HPV have been introduced, millions have been already been exposed so that incidence is expected to rise in the coming decades.
This Company Sponsored Research is provided by Noble Capital Markets, Inc., a FINRA and S.E.C. registered broker-dealer (B/D).
*Analyst certification and important disclosures included in the full report. NOTE: investment decisions should not be based upon the content of this research summary. Proper due diligence is required before making any investment decision.